Day 1
Today was the introduction into the depths of clinical pharmacy. I shadowed the chief clinical pharmacist of St. Luke's Hospital where I joined in on some press conferences. Today was a slow day for most of the pharmacists and anesthesiologists, so they organized some meetings to be held today since they have no cases assigned. They first conference I sat in on was a joint conference of clinical pharmacists and clinicians to update the antibiogram which is used to determine the appropriate antibiotic for a patient. They revised, and updated the documents to better suit the clinicians. My second conference was the Pharmacy and Therapeutics Committee Quarterly Meeting where clinical pharmacists, anesthesiologists, and ER practitioners discuss new drugs they would recommend the hospital to introduce, issues concerning the cost of a drug and why it was used too often, and to share information gathered that could be the cause of an issue. The conference was held with a booklet that would contain charts and data to help determine the effectiveness of the new proposed drug, the cost of it, and the shelf life of it. Overall most of the day was spent in meetings, but it was interesting to see different practitioners indulge and discuss as a group how to make each of their jobs easier and to keep the small hospital running. I also learned how pharmacists decide on what types of drugs to keep in stock for the clinicians to use.
Day 2
Today I spent a lot of time in the pharmacy assisting a pharmaceutical student in filling out a clinical form. The clinical form is a list of patients the system flagged that had an opportunity to change their IV bag to an oral medicine, had low platelets, and for monitoring anticoagulation, warfarin, renal status, and HbA1c levels. After we had read through the list and noted suggestions for the Chief Clinical Pharmacist to take a look at, we spoke to her and gave some comments on what dosage needs to be changed for a patient or if the medication needs to be replaced with a less potent solution. Due to her clearance level, she did not have to notify a physician about the changes, rather, she had access to the patients personal documents and changed them directly, while also making notes she had changed it. We could see if the nurses had given the medication, if it was overdue, or if it was scheduled to be delivered to the patient. Unfortunately, due to there being patient information that is legally protected, I was unable to take any pictures of the list.
After discussing and revising the clinical form, I joined the Chief Clinical Pharmacist for a meeting discussing the addition to a new sector. The new sector would add another hybrid operating room and an electro physiology lab. There was conflict in naming the addition since marketing wise, the hospital was unsure if the new addition would profit or lose money. If the name of the rooms were "Hybrid Operating Room #3" and "Electro Physiology Lab #3" it would be harder to discern how much income the rooms were making than if they were given and independent name.
Soon after the conference, I joined in on a presentation by another pharmaceutical student discussing "Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke". Alteplase and tenecteplase are both thrombolytic agents that bind to fibrin which converts plasminogen to plasmin. Tenecteplase has 3 point mutations from alteplase, making it more fibrin specific, and more resistant to plasminogen activator inhibitor-1. Although tenecteplase is longer lasting and more efficient, it is more specific to a type of isechemic stroke than alteplase, as tenecteplase can only treat 13% of iseschemic stroke patients.
Overall, the day was very exciting and I learned a lot about how practitioners determine what medications are needed for each patient and that it is handled by the clinical pharmacists. I also learned the marketing side of a hospital and how practitioners from different sectors of the hospital communicate with each other. Tomorrow the Chief Clinical Pharmacist will not be there, so I will be shadowing multiple different individuals from different sections of the pharmacy.
After discussing and revising the clinical form, I joined the Chief Clinical Pharmacist for a meeting discussing the addition to a new sector. The new sector would add another hybrid operating room and an electro physiology lab. There was conflict in naming the addition since marketing wise, the hospital was unsure if the new addition would profit or lose money. If the name of the rooms were "Hybrid Operating Room #3" and "Electro Physiology Lab #3" it would be harder to discern how much income the rooms were making than if they were given and independent name.
Soon after the conference, I joined in on a presentation by another pharmaceutical student discussing "Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke". Alteplase and tenecteplase are both thrombolytic agents that bind to fibrin which converts plasminogen to plasmin. Tenecteplase has 3 point mutations from alteplase, making it more fibrin specific, and more resistant to plasminogen activator inhibitor-1. Although tenecteplase is longer lasting and more efficient, it is more specific to a type of isechemic stroke than alteplase, as tenecteplase can only treat 13% of iseschemic stroke patients.
Overall, the day was very exciting and I learned a lot about how practitioners determine what medications are needed for each patient and that it is handled by the clinical pharmacists. I also learned the marketing side of a hospital and how practitioners from different sectors of the hospital communicate with each other. Tomorrow the Chief Clinical Pharmacist will not be there, so I will be shadowing multiple different individuals from different sections of the pharmacy.
Day 3

Today the Chief Clinical Pharmacist was not at the clinic today, so I was unable to shadow her, rather, she organized for me to shadow her colleagues. I started off shadowing a pharmacist assigned to the ICU where she reviews each patient's transcript written up by the physician, and then checks the list of medications they are taking. If there are any changes she would recommend to the dosage or the type of prescription, she takes note if it. Unlike the Chief Clinical Pharmacist, she does not have the necessary clearance to directly change the patients prescription list, so she meets the doctors, dietary nurses, and social workers to discuss changes with the patients. After she reviewed every patient she traveled upstairs to the ICU where she had a meeting with everyone from the ICU. Nurses caring for each patient came with their transcript on the patient and added any new changes to the patients well being. This meeting is where the pharmacist adds any suggestions to the medications the patient should be taking.
After my session with the pharmacist, I was sent to work with a pharmaceutical student working in the ER. He collects all medications given to a patient when they visit to create a medication list perscribed to the patient. He often visits the patient while they are entering a room to ask if they have their prescription list in their head, if they have the sheet on them, or if a family member is soon to bring it. If none of the previous stated is true, then he asks them a series of questions to get a general census of what medications they should need.
Shortly after my visit to the ER, I visited another pharmacist in the clinic who displayed another clinical form that he reviews for patients. However, he specializes in antibiotics, so he focuses on if the patient has been diagnosed with a bacterial infection, which he pinpoints to a specific drug such as Penicillin or Oxacillin. However, most patients who are just admitted to the hospital are not diagnosed with a specific bacterial infection yet, they are only swabbed and then plated where the doctors can get a brief diagnosis as to if they have an infection or not. If they do, the pharmacist often starts off with a more general antibiotic such as Vancomycin until the cultures are fully grown for the bacteria to be identified.
The day was more of a casual, behind the screen day where I observed pharmacists reviewing patients forms. Tomorrow, the Chief Clinical Pharmacist will return, which in hope will allow me to do some more hands on activities such as activating the tube to deliver prescriptions to another patient.
After my session with the pharmacist, I was sent to work with a pharmaceutical student working in the ER. He collects all medications given to a patient when they visit to create a medication list perscribed to the patient. He often visits the patient while they are entering a room to ask if they have their prescription list in their head, if they have the sheet on them, or if a family member is soon to bring it. If none of the previous stated is true, then he asks them a series of questions to get a general census of what medications they should need.
Shortly after my visit to the ER, I visited another pharmacist in the clinic who displayed another clinical form that he reviews for patients. However, he specializes in antibiotics, so he focuses on if the patient has been diagnosed with a bacterial infection, which he pinpoints to a specific drug such as Penicillin or Oxacillin. However, most patients who are just admitted to the hospital are not diagnosed with a specific bacterial infection yet, they are only swabbed and then plated where the doctors can get a brief diagnosis as to if they have an infection or not. If they do, the pharmacist often starts off with a more general antibiotic such as Vancomycin until the cultures are fully grown for the bacteria to be identified.
The day was more of a casual, behind the screen day where I observed pharmacists reviewing patients forms. Tomorrow, the Chief Clinical Pharmacist will return, which in hope will allow me to do some more hands on activities such as activating the tube to deliver prescriptions to another patient.
Day 4
For my last day at the clinical pharmacy, I shadowed the pharmacy technician while the chief clinical pharmacist was off at a meeting. He was eager to show me the rest of the pharmacy that I have not seen, which included being able to send some medications through a tube up to the nurses in the OR which was very exciting. I also toured the rest of the pharmacy with all the medications such as IV's, oral medicines, liquid medications, sedatives, anticoagulants, and colonoscopy cleaners . There was another room inside the pharmacy that contained a system with all the medications stored in the hospital. The pharmacist I was shadowing showed me that it is imperative you keep track of how many pills or doses of each medication there are in the cabinets, otherwise there will be huge issues. All of the cabinets are locked for safety precautions, so if you would like a certain medication, you search it up on the computer, and the cabinet containing the medication opens. If you would like to withdraw, you must update the total number of pills there now are in the cabinet to keep inventory. If you incorrectly count the total number two times consecutively, the computer flags that drawer, and the pharmacist has to view the report and see if it was off by a huge or minor margin.
I then followed the Chief Clinical Pharmacist to a meeting held by another pharmacist I shadowed the day before. He is the pharmacist that mainly specializes in antibiotics, so there was a press meeting that changed some online fill out forms to a more detailed check list. The illnesses addressed were influenza and pneumonia.
I also was able to discuss with the two student pharmacists and the chief clinical pharmacist about the transition from high school to college, which was very insightful and informative. I now have a deeper understanding about the workload in a university compared to a high school.
Finally, I was able to sit in on an interview for a part-time job as a technician who was interviewed by one lead pharmacist and the chief clinical pharmacist. Due to this individual being the only applicant for the role, as long as he does not signal any red flags, he should have a good chance at receiving the job. However, he had just left a full-time job and is now seeking out another full-time job which unfortunately St. Luke's does not provide at the moment, so the chief clinical pharmacist was keen on making sure he was not going to go through 4 weeks of extensive training just to leave the clinic in the following two months to come.
Overall, this entire week was a huge experience with me that I could not have learned in a classroom setting. Every individual I shadowed was kind and always open to answer questions. And considering I am shadowing them doing their job, they were surprisingly very interactive with me and always allowing me to pitch in on the work they are doing. I was gladly able to visit almost every aspect of the pharmacy environment, and am now familiarized with the pharmacy and the jobs that come with it. I thank the chief clinical pharmacist for taking me in and showing me a countless number of interesting experiences I will never forget. I just hope my next week in the Emergency Room will be as immersive as this past week, and we will see if I have the stomach to handle being in the ER.
I then followed the Chief Clinical Pharmacist to a meeting held by another pharmacist I shadowed the day before. He is the pharmacist that mainly specializes in antibiotics, so there was a press meeting that changed some online fill out forms to a more detailed check list. The illnesses addressed were influenza and pneumonia.
I also was able to discuss with the two student pharmacists and the chief clinical pharmacist about the transition from high school to college, which was very insightful and informative. I now have a deeper understanding about the workload in a university compared to a high school.
Finally, I was able to sit in on an interview for a part-time job as a technician who was interviewed by one lead pharmacist and the chief clinical pharmacist. Due to this individual being the only applicant for the role, as long as he does not signal any red flags, he should have a good chance at receiving the job. However, he had just left a full-time job and is now seeking out another full-time job which unfortunately St. Luke's does not provide at the moment, so the chief clinical pharmacist was keen on making sure he was not going to go through 4 weeks of extensive training just to leave the clinic in the following two months to come.
Overall, this entire week was a huge experience with me that I could not have learned in a classroom setting. Every individual I shadowed was kind and always open to answer questions. And considering I am shadowing them doing their job, they were surprisingly very interactive with me and always allowing me to pitch in on the work they are doing. I was gladly able to visit almost every aspect of the pharmacy environment, and am now familiarized with the pharmacy and the jobs that come with it. I thank the chief clinical pharmacist for taking me in and showing me a countless number of interesting experiences I will never forget. I just hope my next week in the Emergency Room will be as immersive as this past week, and we will see if I have the stomach to handle being in the ER.
Day 5
Working at the ER is an immensely different experience than working at the pharmacy. You get much more human interaction, and, at the ER, everyone can visit and are required by law to be taken in under care. This means that you can see some of the strangest patient descriptions come in such as Facial Swelling, Suicidal Ideation, Abdominal Pain, and Portacath Line Infection. The ER is not specialized in any way. Doctors at the ER do not perform any major life changing surgeries there either. Unlike most interpretations of hospitals, the ER is there to treat and keep a patient alive and stable enough to be transferred off to different sectors at the hospital, or even a different hospital. I was able to shadow one of the two doctors on call today, and his routine consists of accepting patient's in when admitted to a room (which is often based on severity), do a well check which consists of feeling different areas of a patient's trauma region for indication of a fracture or bruise. The rating for severity is from 1-5. 1 is the most severe and often never utilized unless the patient is sure to die without immediate attention. Today there were no patients with the rating of 1, so the main routine did consist of checkups. After the physician does a checkup, the labs soon come back testing for white blood cell count, Creatinine levels, Platelet count, phosphorous levels, etc. The physician views these forms in case of any abnormalities in levels that could be dangerous. Otherwise, he just prescribed them some antibiotics, pain relief medications and then discharged them from the rooms to open up new spaces in the ER. Otherwise, there might be some small operations for the patients such as an embedding of the central line, which I observed today.
I also asked the doctor I shadowed today how he operates on a daily basis at the ER, and he replied, "it's like tying shoes. You create a routine of how you tie your shoes which does not change by day, and eventually, you become more and more efficient at it. Eventually, you even forget you tie your shoes because it falls into your unconscious mind". After what he told me, I observed for the rest of the day what he meant by that. In reality, doctors treat every patient they recieve the same. There might be minor changes to your routines depending on the severity or type of problem the patient has, but, often your routine stays the same throughout. That is how ER Doctors are able to breeze through patients as quick as possible to get in the next set of patients with as minimal amount of time waiting as possible.
The first day at the ER was stressful. I did not expect it to become that busy due to when I came in, we only saw 1 or 2 patients every hour until 11:00. Then, at 11:00, we were hit with 8-9 patients ever hour until 1:00. It was hectic. With only two doctors on call, they had to reduce the amount of time spent on a patient by 75% to make sure they got to everyone. The work, however, was not arduous, it was exciting. Seeing all the different variations of patients with different illnesses and the severity differ was very interesting. I will be shadowing a different practitioner tomorrow, as the one I shadowed today will not be in.
I also asked the doctor I shadowed today how he operates on a daily basis at the ER, and he replied, "it's like tying shoes. You create a routine of how you tie your shoes which does not change by day, and eventually, you become more and more efficient at it. Eventually, you even forget you tie your shoes because it falls into your unconscious mind". After what he told me, I observed for the rest of the day what he meant by that. In reality, doctors treat every patient they recieve the same. There might be minor changes to your routines depending on the severity or type of problem the patient has, but, often your routine stays the same throughout. That is how ER Doctors are able to breeze through patients as quick as possible to get in the next set of patients with as minimal amount of time waiting as possible.
The first day at the ER was stressful. I did not expect it to become that busy due to when I came in, we only saw 1 or 2 patients every hour until 11:00. Then, at 11:00, we were hit with 8-9 patients ever hour until 1:00. It was hectic. With only two doctors on call, they had to reduce the amount of time spent on a patient by 75% to make sure they got to everyone. The work, however, was not arduous, it was exciting. Seeing all the different variations of patients with different illnesses and the severity differ was very interesting. I will be shadowing a different practitioner tomorrow, as the one I shadowed today will not be in.
Day 6
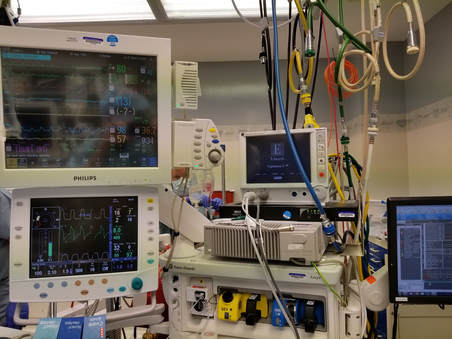
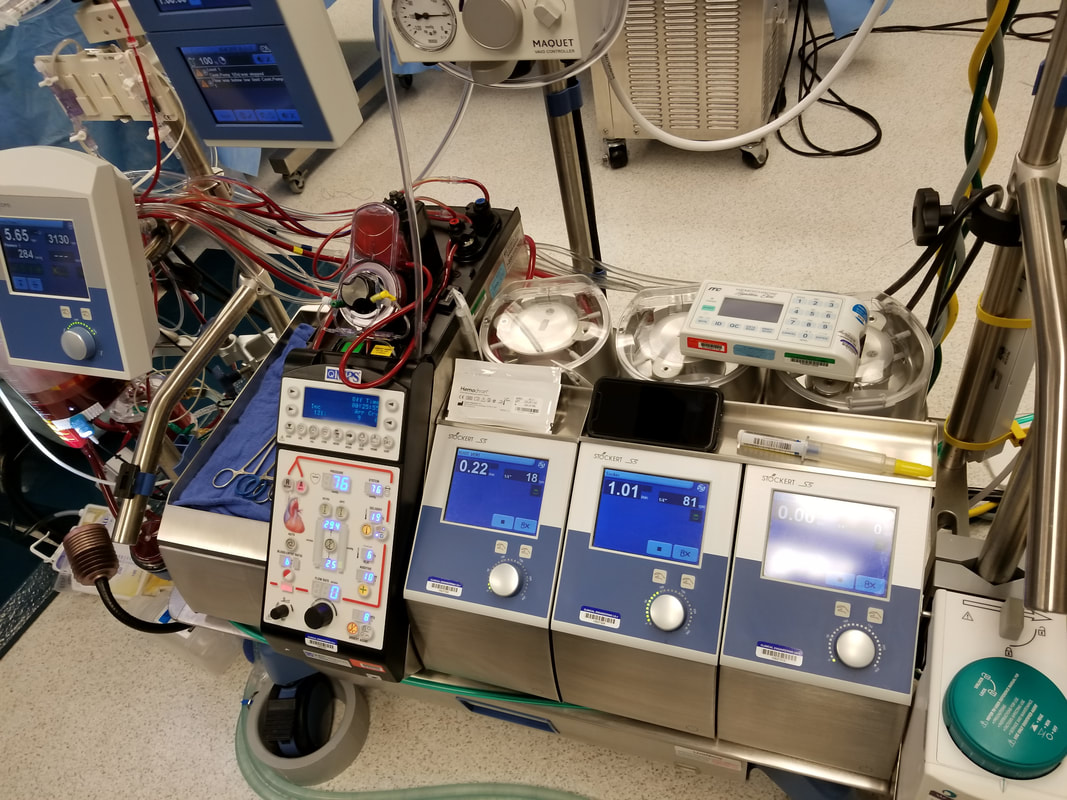
The late morning to mid afternoon at the ER was running a little slow, so I was offered to visit the CVOR to see an ongoing surgery that involved a patient who had myocardial ischemia and was undergoing coronary bypass surgery. It involves attaching a new vessel beyond the blockage of the native heart vessel. This type of operation is typically done on a non-beating heart which requires an artificial heart-lung machine. They remove the heart, attach a new vessel rerouting circulation, reinsert the heart, and stimulate it again for revival of the heart. The procedure is done under general anesthesia while the patient's heart is being actively evaluated by a trans esophageal echo (TEE). I was able to stand at the head of the patient watching over with 9 other individuals scattered across the room, 5 on the patient. The cardio thoracic surgeon on call was very kind to explain to me what was actively occurring. After the surgery, I returned to the ER which then had an active amount of individuals flowing in. Today, I shadowed a different ER doctor who was also very explanatory in the types of issues being addressed. Today I saw examples of Leg pain/swelling, Tailbone injury, left chest pain, lip through and through, chemical exposure, face numbness, and leg swelling. Of all of these diagnoses, only one required a procedure other than basic antibiotics and pain relievers, which was the lip through and through. A poor 4 year old boy was out at the park and fell face first onto a metal staircase smashing his tooth into the bottom lip cutting all the way through. After some general anesthesia, the ER doctor sutured the lip closed on both ends. Listening to a child being sutured while still awake is a very big difference to an adult, as they do not understand they cannot feel anything during the procedure, they just understand something painful is going on. It was a very different experience to others I listened in on. I really enjoyed visiting the CVOR as it was more than a basic operation you see at an ER for example. These are not only doctors, but ones who spent even more time studying in on specific fields to perform surgeries such as a coronary bypass surgery. All of the information being displayed at once was overwhelming, yet I was able to comprehend some of what was going on. I had some help from the other nurses and physicians in the OR. The ER is showing me that many individuals visiting just would like answers to their issues immediately, while, they don't realize that is not what ER doctors do. ER doctors are specialized to keep you stable and alive long enough to discharge you home or to another area at the hospital. You should not visit an ER unless you need serious medical attention or are severely worried about a problem. Otherwise, visiting Urgent Care would be the best idea, as it is not nearly as expensive and you would have better chances at fixing a small issue.
Day 7
The ER was running surprisingly slow today which appeared confusing to everyone in the ER. However, as the ER doctor I was shadowing said, "We have a saying around here for us ER doctors, never say there aren't many patients coming in because then, when you are being overwhelmed with work will you regret ever saying it". We were still able to see some more serious conditions of patients contradictory to the patients we saw yesterday which consisted of people wanting answer. The highlights I saw today were: A patient with Pleveritic pain, Atelectasis, Hypoxia, and Pneumonia. A patient with a Dextrothemorphan overdose from mucinex DM consuming 32 pills each 60 mg which caused urinary retention and serotonin syndrome. And a patient with chest pain, hypertension, mild dehydration, and renal insufficiency (creatinine clearance was abnormally low). The visit with the OD patient was very unique as he was only 19 years old and was staying at a sober living facility due to his methamphetamine addiction, which then he went to a pharmacy and bought the over the counter drug mucinex DM. He overdosed yesterday at 4:00 and he arrived at the ER at noon. He seemed overly groggy and agreed with every question the doctor asked. To test for serotonin syndrome, the doctor showed me his procedure of holding up one finger and moving it back and forth in front of the patient asking for him to follow the finger with his eyes. The twitching of the eyes after stopped was a clear sign of serotonin syndrome which brought immediate attention to him considering serotonin syndrome is one of the more deadly syndromes in the ER. Overall, not a too busy or exciting day unfortunately. I also checked in on the CVOR to see if I could shadow any cases but there were none scheduled. There are two scheduled for tomorrow that I can attend so I hope to be able to visit. I got some good explanations of the relevance of an EKG and the importance of placing sticky pads in certain locations on a patient. I will be glad to share on my final presentation! Tomorrow the ER doctor scheduled for 8-8 is the same one I shadowed on monday, so it will be nice to shadow a familiar doctor. We will see how busy the ER will be on a thursday.

Day 8
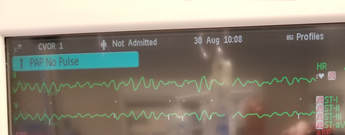
I visited another surgical operation today which was a coronary bypass surgery. Last time I came too late to observe the heart being put to sleep while the heart-lung machine was operating for both the hear and lung. This time, I also saw a nurse preparing the bypass they use for the rerouting of the aorta blockage. The description is the same as it looks in real life. The surgeon stitches the bypass onto the outside of the heart around the blockage to reroute the blood. I also took some photos of the EKG displaying what is called a "dead man's rhythm". A "dead man's rhythm" is when the heart has no rhythm to beating, rather, it is just pulsating randomly similar to the motions you would see from a dying animal. I also spoke with the Perfusionist (Cardiopulmonary Bypass Doctor) who explained to me all of the different parts of a heart-lung machine. For example, there is a little propeller that rotates at around 3000 rpm to mimic the pressure the blood would receive when passing through the heart. It is then cycled through some more tubes where the oxygen is pulled from the blood into what would be the artificial lung. Most of the other parts are just to mimic the pulsation of the heart, and he has access to a panel which allows him to control the blood pressure for when the surgeon asks to lower it –due to an incision bleeding– which slows down the flow of blood to the cut.
The ER had some interesting cases such as a patient who was 41 years old weighing around 75 pounds coming in due to alcohol intoxication. Her blood alcohol concentration was .48 when she arrive. It was a miracle she even made it to the hospital. They treated her with some bolus which drained quite quickly. She ended up going through 5 bolus IV's in the hour. Her BAC eventually decreased due to dilution, and she is now being admitted to a rehab facility to monitor her drinking. There was another patient with a cyst on the back of his neck which is treated with some Lidocaine injected into the cyst and then the ER doctor makes an incision in the surface and puts pressure on the wound to remove any dead white blood cells (pus) or red blood cells (blood). After, you would assume he sealed the wound up with some sutures to prevent any new bacteria from entering the opening and causing another cyst, however, he instead inserted a gauze into the opening and left it inside. The reason for this is because they want the opening to regenerate from the inside to the outside to prevent any new bacteria from entering the body. Of course, the gauze would need to be replaced every 2-3 days until the wound is fully healed.
The day was very interesting as this time I got to sit in on another open heart surgery, although similar, I still was able to observe some new parts to the procedure I missed the first time around. I will be able to sit in on another open heart surgery tomorrow where I will finally arrive at the beginning of the surgery to see the central line put in the patient, and the incision above the heart made. The same ER doctor will be there tomorrow, and I hope we can wrap up any questions I have about the ER for my final day. I realized now at this point many of the patient visits do no need to happen at the ER as they are not life threatening. However, the doctors are there for the one time a patient comes in with severe need of help.
The ER had some interesting cases such as a patient who was 41 years old weighing around 75 pounds coming in due to alcohol intoxication. Her blood alcohol concentration was .48 when she arrive. It was a miracle she even made it to the hospital. They treated her with some bolus which drained quite quickly. She ended up going through 5 bolus IV's in the hour. Her BAC eventually decreased due to dilution, and she is now being admitted to a rehab facility to monitor her drinking. There was another patient with a cyst on the back of his neck which is treated with some Lidocaine injected into the cyst and then the ER doctor makes an incision in the surface and puts pressure on the wound to remove any dead white blood cells (pus) or red blood cells (blood). After, you would assume he sealed the wound up with some sutures to prevent any new bacteria from entering the opening and causing another cyst, however, he instead inserted a gauze into the opening and left it inside. The reason for this is because they want the opening to regenerate from the inside to the outside to prevent any new bacteria from entering the body. Of course, the gauze would need to be replaced every 2-3 days until the wound is fully healed.
The day was very interesting as this time I got to sit in on another open heart surgery, although similar, I still was able to observe some new parts to the procedure I missed the first time around. I will be able to sit in on another open heart surgery tomorrow where I will finally arrive at the beginning of the surgery to see the central line put in the patient, and the incision above the heart made. The same ER doctor will be there tomorrow, and I hope we can wrap up any questions I have about the ER for my final day. I realized now at this point many of the patient visits do no need to happen at the ER as they are not life threatening. However, the doctors are there for the one time a patient comes in with severe need of help.
Day 9
My final visit for a coronary bypass surgery gave me the full experience of one surgery. Every coronary bypass surgery starts with a central line insertion. The trans esophageal echo (TEE) then probes the patient to investigate all of the different valves of the patient's heart. Presumably, this patient's aortic valve is severely damaged. Since I have not seen the interior of a healthy heart, I have no reference point. Yet, it is still noticeable that the movement of the valve is minuscule and distraught.
Today at the ER, there was a patient who came in for some abdominal pain near their appendix. The ER doctor assumed it was appendicitis, so they performed a CT scan to investigate the area. Surprisingly, there were no clear signs that indicated the patient had appendicitis. There was apparently a kidney stone in the patient that had just passed while they were at the ER. The patient neglected to say anything about him passing two stones previously while currently at the age of 18, and that his family had a history of kidney stones. There was another patient with Submassive Pulmonary Embolism, meaning there are clots in the lungs which can cause chronic pulmonary hypertension, persistent right ventricular dysfunction, and recurrent venous thromboembolism. They can treat this with a new procedure that is FDA approved called Optimum Duration and Dose of r-tPA with the Acoustic Pulse Thrombolysis Procedure (OPTALYSE PE). This procedure involves inserting an infusion catheter into the clot, and then fitting an ultrasonic core in the center of the infusion catheter, which will pulsate ultrasound waves which signals the blood cells to rejoin in a different order, thus declotting the ldungs at the source.
Overall, my final day at the Emergency Room was similar to most days at the ER. I learned at my time there that it is not as unique as people would suspect due to the stereotype television shows give the ER. Rather, most patients that visit the ER are not near death, rather, it is some minor injury that they would like answers to, which ER doctors do not do. So if you face the same issue, do not visit the ER for answers, you will find none. The doctors I shadowed at the ER were very informative which is very nice considering it is different to shadowing a pharmacist who has a whole day to fill out their clinical forms. A doctor needs to keep a fast pace during the day to visit every patient and treat them. Doing all of those things while also explaining what is happening to me is very thoughtful and tiring. I hope I did not annoy them while I was there! Of course I thank them all for letting me visit. Tomorrow I will be observing with an Interventional Cardiologist who will be performing cardiac catheterizations in the Cath lab. This includes diagnostic heart lesions and/or treatment of coronary disease. Hopefully they will be explanatory in the process of diagnostic heart lesions and what each step is to the catheterization.
Today at the ER, there was a patient who came in for some abdominal pain near their appendix. The ER doctor assumed it was appendicitis, so they performed a CT scan to investigate the area. Surprisingly, there were no clear signs that indicated the patient had appendicitis. There was apparently a kidney stone in the patient that had just passed while they were at the ER. The patient neglected to say anything about him passing two stones previously while currently at the age of 18, and that his family had a history of kidney stones. There was another patient with Submassive Pulmonary Embolism, meaning there are clots in the lungs which can cause chronic pulmonary hypertension, persistent right ventricular dysfunction, and recurrent venous thromboembolism. They can treat this with a new procedure that is FDA approved called Optimum Duration and Dose of r-tPA with the Acoustic Pulse Thrombolysis Procedure (OPTALYSE PE). This procedure involves inserting an infusion catheter into the clot, and then fitting an ultrasonic core in the center of the infusion catheter, which will pulsate ultrasound waves which signals the blood cells to rejoin in a different order, thus declotting the ldungs at the source.
Overall, my final day at the Emergency Room was similar to most days at the ER. I learned at my time there that it is not as unique as people would suspect due to the stereotype television shows give the ER. Rather, most patients that visit the ER are not near death, rather, it is some minor injury that they would like answers to, which ER doctors do not do. So if you face the same issue, do not visit the ER for answers, you will find none. The doctors I shadowed at the ER were very informative which is very nice considering it is different to shadowing a pharmacist who has a whole day to fill out their clinical forms. A doctor needs to keep a fast pace during the day to visit every patient and treat them. Doing all of those things while also explaining what is happening to me is very thoughtful and tiring. I hope I did not annoy them while I was there! Of course I thank them all for letting me visit. Tomorrow I will be observing with an Interventional Cardiologist who will be performing cardiac catheterizations in the Cath lab. This includes diagnostic heart lesions and/or treatment of coronary disease. Hopefully they will be explanatory in the process of diagnostic heart lesions and what each step is to the catheterization.
Day 10

Today I visited the Cath lab and shadowed a Medtronic LINQ loop recorder insertion. A loop recorder is an EKG monitor that gathers heart rhythm data from the loop recorder and sends it to St. Luke's. The procedure starts with preparation and then the patient is draped, a common procedural sterile step of any hospital. Then, Lidocaine is administered to the chest where the loop recorder is going to be inserted. The Medtronic LINQ loop recorder is then inserted via an incision just above the left upper quadrant of the abdomen, and then a tool with the loop recorder inside is then inserted in the incision which then properly places the loop recorder inside the patient. The patient can then record any periods of time for the loop recorder to save which will then send to St Luke's at its routine checkup date which is often every weekend. Since the loop recorder is limited in storage, it only saves certain bits of information that it notices as abnormal, or if the patient records a sequence. Priority comes to the machine detecting anything rather than the patient in terms of storage.
During my time in the Cath Lab, I also observed a ventricular tachycardia patient who came in for a radial catheterization. This patient in fact had a Medtronic loop recorder which detected a severely abnormal blood pressure in the pulmonary valve which can send an automatic alert to the hospital. The physician I shadowed saw the alert and notified the patient to visit the hospital immediately. The catheterization allows for him to properly examine the different areas of the patient's heart for any abnormalities in pressure or valve function. After catheterization, the doctor decided on an iFR line insertion to test for a pressure differential in the left ventricle. Studies have shown that abnormalities in pressure only needs treating if there is an 11% decrease in pressure. Anything less than 11% does not require treatment. Treatment consists of coronary heart bypass to avoid the clot in the left ventricle, or other anticoagulants in hopes of the clot dissipating on its own.
Due to the doctor I shadowed today having some early meetings, I visited him at 11:00. From 8-11 I was back at the ER shadowing some more cases. Out of my entire week at the ER, I had not seen a priority 1 case which is when a patient is near death and requires immediate attention from the medical staff (i.e. drop what you are doing). Today, however, a 15 year old female came in with a Benadryl overdose and was unresponsive. Routine services would've consisted of a lavage which is removal of any consumed particles inside the bowel, however, the patient was unconscious and unresponsive, so that indicated that the Benadryl had already dissolved and was too late for a lavage. So, the only proper processes they could perform was some general anesthesia and some anticoagulants to help settle the patient's heart rate down, and then to transfer off to the ICU.
Overall the day was quite exciting. I got to experience a new field while also seeing some serious cases today at the short time I spent at the ER. I also learned about the iFR scale which is the main determinant for a patient to have open heart surgery, and I also was able to see some live feeds of veins pumping blood. It is unique that during the operation the patients are not sedated during the procedure but just administered some light anesthesia to numb the arm. It was a nice short experience I was able to visit at the hospital to understand the first step to a patient admitted to the CVOR.
During my time in the Cath Lab, I also observed a ventricular tachycardia patient who came in for a radial catheterization. This patient in fact had a Medtronic loop recorder which detected a severely abnormal blood pressure in the pulmonary valve which can send an automatic alert to the hospital. The physician I shadowed saw the alert and notified the patient to visit the hospital immediately. The catheterization allows for him to properly examine the different areas of the patient's heart for any abnormalities in pressure or valve function. After catheterization, the doctor decided on an iFR line insertion to test for a pressure differential in the left ventricle. Studies have shown that abnormalities in pressure only needs treating if there is an 11% decrease in pressure. Anything less than 11% does not require treatment. Treatment consists of coronary heart bypass to avoid the clot in the left ventricle, or other anticoagulants in hopes of the clot dissipating on its own.
Due to the doctor I shadowed today having some early meetings, I visited him at 11:00. From 8-11 I was back at the ER shadowing some more cases. Out of my entire week at the ER, I had not seen a priority 1 case which is when a patient is near death and requires immediate attention from the medical staff (i.e. drop what you are doing). Today, however, a 15 year old female came in with a Benadryl overdose and was unresponsive. Routine services would've consisted of a lavage which is removal of any consumed particles inside the bowel, however, the patient was unconscious and unresponsive, so that indicated that the Benadryl had already dissolved and was too late for a lavage. So, the only proper processes they could perform was some general anesthesia and some anticoagulants to help settle the patient's heart rate down, and then to transfer off to the ICU.
Overall the day was quite exciting. I got to experience a new field while also seeing some serious cases today at the short time I spent at the ER. I also learned about the iFR scale which is the main determinant for a patient to have open heart surgery, and I also was able to see some live feeds of veins pumping blood. It is unique that during the operation the patients are not sedated during the procedure but just administered some light anesthesia to numb the arm. It was a nice short experience I was able to visit at the hospital to understand the first step to a patient admitted to the CVOR.
Day 11
The individual I shadowed today was a Registered Diagnostic Cardiac Sonographer at the Echo Lab. I viewed live Echo feeds of patient's hearts while also viewing some past interesting cases the Sonographers saved. The cases consisted of thrombi, cysts, and vegetation. I saw one case with a patient who had a serious vegetation growth on the tricuspid valve and if it detached, a possible fatal stroke could occur. The vegetation had completely overwhelmed the tricuspid valve destroying its function causes a lot of regurgitation of blood flow. The only option the patient had was for complete replacement of the valve. Unfortunately, this patient was only 20 years old. The reason for this serious case of vegetation growth is due to drug use. The patient was a heroin addict, which can flow into the blood and collect inside the heart on valves. A TEE was requested for the patient which is what detected the growth in the heart. TEE's are inserted into the patients throat down towards the heart for a clearer view of all of the valves and ventricles. A regular echo would be placed on the surface of a patient's chest which would have to pass through all of the tissue, bone, and muscle before reaching the heart causing a less clear picture. Any clots the regular echo can detect would be flagged for removal as any abnormal growths that can be seen on the echo is large enough for concern.
I also sat in on an echo with a patient who required definity for a clearer picture. Usually more obese individuals have more fat around the heart which can cloud the pictures. Definity is a small medication inserted via IV which will color the outer walls of the heart which clears up the picture. The sonographers have this small machine which vibrates the definity at a fast rate to cycle the fluid before they insert it. I was explained each section of the hearts and what parts are recorded for review. Some are captured in 1D for a cross section view of the heart to view a ventricle contracting. Some ventricles and atriums are recorded with a heat sensor to capture blood flow for any abnormalities in the severity of the regurgitation.
I learned all of the procedures a sonographer does to capture all of the photos of the heart for the doctor to review. I also was shown the form they fill out after looking over their own photos which answers any questions the doctors requested. The two sonographers I shadowed were very kind and helpful in explaining everything they are doing. It is a little easier to follow what they are doing as there are no overly complicated terms used, and I only would need to understand the different section of the heart excluding vascular. Tomorrow I will be shadowing a Radiologist to view some CT, CAT, and MRI scans. The ER doctors and cardiovascular surgeons did some interpretations of the scans, however, shadowing a Radiologist who specializes in reading scans will really help me notice abnormalities in scans. I hope it will be exciting!
I also sat in on an echo with a patient who required definity for a clearer picture. Usually more obese individuals have more fat around the heart which can cloud the pictures. Definity is a small medication inserted via IV which will color the outer walls of the heart which clears up the picture. The sonographers have this small machine which vibrates the definity at a fast rate to cycle the fluid before they insert it. I was explained each section of the hearts and what parts are recorded for review. Some are captured in 1D for a cross section view of the heart to view a ventricle contracting. Some ventricles and atriums are recorded with a heat sensor to capture blood flow for any abnormalities in the severity of the regurgitation.
I learned all of the procedures a sonographer does to capture all of the photos of the heart for the doctor to review. I also was shown the form they fill out after looking over their own photos which answers any questions the doctors requested. The two sonographers I shadowed were very kind and helpful in explaining everything they are doing. It is a little easier to follow what they are doing as there are no overly complicated terms used, and I only would need to understand the different section of the heart excluding vascular. Tomorrow I will be shadowing a Radiologist to view some CT, CAT, and MRI scans. The ER doctors and cardiovascular surgeons did some interpretations of the scans, however, shadowing a Radiologist who specializes in reading scans will really help me notice abnormalities in scans. I hope it will be exciting!
Day 12
Today I shadowed a Radiologist to watch some reviews of some MRI, CT, CAT, and X-ray scans. Any types of scans that involve any body part are transferred to a list the Radiologists review. The Radiologists that work for St. Luke's are independent. There are a total of 35 Radiologists that coordinate together and work at St. Luke's and any Promedica Hospital. The stereotype of how a radiologist operates is indistinguishable from what I shadowed. It is unique because the new screens radiologists use, which can allow for the lights to be on. However, radiologists are used to the habits of sitting in a dark room for 8 hours that they are fine with keeping them off, even if unnecessary.
The time I spent with the radiologist had a lot of cases come up with a lumbar MRI. The radiologist I spoke with said they have a strong dislike for the reports of lumbar MRI's due to the radiologist having to write up a description for each vertebrae from T-12 to S1 which is a total of 7 vertebrae. The analysis of the lumbar is very simple, but the whole process is tedious making the reports very boring. I also heard from the radiologist that abdominal MRI's are near useless for analysis as they do not show the radiologist anything. The only reason abdominal MRI's are even administered is due to patient's complaining about abdominal pain, and not doing any MRI scans seems inappropriate and it keeps the patient happy with receiving some sort of treatment.
Along with general analysis of any type of scan, this radiologist also looks at mammography digital screening scans. Some statistics he told me was that only around 5-9 patients out of 1000 are diagnosed with breast cancer during this screening. Due to such a low number, there is a lot of controversy about whether it is worth it to do the screening and expose a large number of women to radiation which could cause breast cancer on its own. Along with the 5-9 patients diagnosed, only 1 out of 22 patients are called back for another screening due to a concern about a lymph node. A new requirement by law now with these screening is that for each patient screened, a short description of the patient's breasts are required. Apparently some patient's breasts were too dense for the radiologists to detect some deeper lymph nodes, and after the screening, they were diagnosed with breast cancer. In response, 32 states passed a legislation that mandates a description of the patient's breasts to notify them that they may require more screening. Unfortunately, any insurance agency only pays for the first set of testing, and there was no law that requires insurance companies to pay for any extra screening required. So, if a patient wants more screening, they would be paying out of pocket.
My experience with the Radiologist was very interesting. They are unalike many of the other professions I shadowed as there is no contact with any of the patients. And, radiologists are never on call, so there is no urgency for them to complete any scripts. Radiology is also more of a general profession similar to the ER, so they need only a general understanding of human anatomy. Some radiologists of course specialize in some fields of medicine which transfers their screening to a certain set of patients. Radiology does not seem as interesting to me as an observer, but as I spoke with the radiologist, he told me that it is a different experience shadowing a radiologist than personally analyzing the scans which makes perfect sense. So, my whole experience today was very unique and different and I am glad I was able to stop by and shadow a different field of expertise.
The time I spent with the radiologist had a lot of cases come up with a lumbar MRI. The radiologist I spoke with said they have a strong dislike for the reports of lumbar MRI's due to the radiologist having to write up a description for each vertebrae from T-12 to S1 which is a total of 7 vertebrae. The analysis of the lumbar is very simple, but the whole process is tedious making the reports very boring. I also heard from the radiologist that abdominal MRI's are near useless for analysis as they do not show the radiologist anything. The only reason abdominal MRI's are even administered is due to patient's complaining about abdominal pain, and not doing any MRI scans seems inappropriate and it keeps the patient happy with receiving some sort of treatment.
Along with general analysis of any type of scan, this radiologist also looks at mammography digital screening scans. Some statistics he told me was that only around 5-9 patients out of 1000 are diagnosed with breast cancer during this screening. Due to such a low number, there is a lot of controversy about whether it is worth it to do the screening and expose a large number of women to radiation which could cause breast cancer on its own. Along with the 5-9 patients diagnosed, only 1 out of 22 patients are called back for another screening due to a concern about a lymph node. A new requirement by law now with these screening is that for each patient screened, a short description of the patient's breasts are required. Apparently some patient's breasts were too dense for the radiologists to detect some deeper lymph nodes, and after the screening, they were diagnosed with breast cancer. In response, 32 states passed a legislation that mandates a description of the patient's breasts to notify them that they may require more screening. Unfortunately, any insurance agency only pays for the first set of testing, and there was no law that requires insurance companies to pay for any extra screening required. So, if a patient wants more screening, they would be paying out of pocket.
My experience with the Radiologist was very interesting. They are unalike many of the other professions I shadowed as there is no contact with any of the patients. And, radiologists are never on call, so there is no urgency for them to complete any scripts. Radiology is also more of a general profession similar to the ER, so they need only a general understanding of human anatomy. Some radiologists of course specialize in some fields of medicine which transfers their screening to a certain set of patients. Radiology does not seem as interesting to me as an observer, but as I spoke with the radiologist, he told me that it is a different experience shadowing a radiologist than personally analyzing the scans which makes perfect sense. So, my whole experience today was very unique and different and I am glad I was able to stop by and shadow a different field of expertise.
Day 13
In the early morning I shadowed a Respiratory Therapist. I was given a quick explanation of everything they do. In short, Respiratory Therapists are specialized nurses that work in the ICC. They are not entirely nurses as they have more qualifications, but not as many as a doctor. Respiratory Therapists keep the patients alive and rush them from different areas of the hospital to one of their respiratory machines. They keep the flow of oxygen to their lungs pure, and at certain amounts they must humidify the oxygen or else it will dry out the patient's nose. They also perform Oxygen Therapy which is an Aerosol Treatment that helps clear out the patient's lungs. The Aerosol treatment only lasts for 5 minutes but is repeated every 12 hours. During the Aerosol treatment, the RT's monitor the sound of the patient's lungs using a stethoscope for any abnormalities in breathing such as jittering, roughness, short inhalation, and prolonged rest. It was a time I was able to spend with them as they are the primary caretakers keeping all the patients healthy.
After my time with the Respiratory Therapist I then shadowed a Pulmonary Disease Specialist. There were 2 scheduled bronchoscopies to occur in the afternoon. Prior to the bronchoscopy, I spoke with the physician who gave me a brief anatomical overview of the lungs and what he will be doing during the bronchoscopy. We reviewed some CT scans of the patient's lungs where he was also able to show me a CT of healthy lungs and compare the two images. To identify a healthy lung, the lungs must span down the chest so that it sits beneath 9 sets of ribs. The patient we viewed had 4 visible. Also, the collarbone should be symmetrical to the vertebrae on both ends, the right side was slightly more angled upward. And lastly the diaphragm should be visible in the CT scan. The patient's right side was visible however it was clouded on the left. I assume due to all these issues are why he has been admitted to the ICC. After my overview came the time for the bronchoscopies. The nurses prepare everything prior to the physician entering the room, so when I entered we were ready to begin. The scope has a vacuum attached to it which can either suck fluids out or put fluids in. The scope enters through the trachea down the left lung first. We go through the lingula where the PDS captures some images of different lobes. He also clears some fluids and collects it in a tube which will later be sent to the lab for testing. After clearing the left lung, the PDS runs through the right middle lobe. Again, photos are taken of all of the lobes which appear abnormal to him. Some areas, the PDS pours some saline in the lobes to clear any mucus or excess fluids. Right after the first bronchoscopy came another, however, there were some issues beginning the procedure. Every patient needs a consent given by a close family member before beginning the procedure. The PDS contacted the wife of the patient 15 minutes prior to the bronchoscopy as he already spoke to her in person the day before. He received no answer from her so then he contacted the son of the patient. Again, there was no answer. As by normal protocol he waited 5 minutes post the scheduled time for the bronchoscopy but still received no answer. Unfortunately, due to no consent given, the bronchoscopy would have to be delayed to another date. It was urgent the patient needed a bronchoscopy but it was not emergent. Only if it is emergent would it be legal for the physician to override the unanswered consent and perform the bronchoscopy as the wife did allow for invasive procedures on the patient.
I was fortunately able to see one bronchoscopy today which the doctor was very informative to me throughout the procedure of what I was seeing on the monitor. Shadowing the Respiratory Therapists was also very interesting, however, due to the Respiratory Therapists having two students shadowing her, I was unable to have very many things explained to me. I completely understand the circumstance, and she was kind enough to realize I was not getting the full experience and let me shadow a free therapist. It is unfortunate I am not able to spend more than one day at the ICC as I definitely did not see all of the procedures a Pulmonary Disease Specialist would do. And, considering the PDS was very kind and outgoing, I am sure I would have learned much from shadowing for a couple of days. I am glad I was able to experience what I can though!
After my time with the Respiratory Therapist I then shadowed a Pulmonary Disease Specialist. There were 2 scheduled bronchoscopies to occur in the afternoon. Prior to the bronchoscopy, I spoke with the physician who gave me a brief anatomical overview of the lungs and what he will be doing during the bronchoscopy. We reviewed some CT scans of the patient's lungs where he was also able to show me a CT of healthy lungs and compare the two images. To identify a healthy lung, the lungs must span down the chest so that it sits beneath 9 sets of ribs. The patient we viewed had 4 visible. Also, the collarbone should be symmetrical to the vertebrae on both ends, the right side was slightly more angled upward. And lastly the diaphragm should be visible in the CT scan. The patient's right side was visible however it was clouded on the left. I assume due to all these issues are why he has been admitted to the ICC. After my overview came the time for the bronchoscopies. The nurses prepare everything prior to the physician entering the room, so when I entered we were ready to begin. The scope has a vacuum attached to it which can either suck fluids out or put fluids in. The scope enters through the trachea down the left lung first. We go through the lingula where the PDS captures some images of different lobes. He also clears some fluids and collects it in a tube which will later be sent to the lab for testing. After clearing the left lung, the PDS runs through the right middle lobe. Again, photos are taken of all of the lobes which appear abnormal to him. Some areas, the PDS pours some saline in the lobes to clear any mucus or excess fluids. Right after the first bronchoscopy came another, however, there were some issues beginning the procedure. Every patient needs a consent given by a close family member before beginning the procedure. The PDS contacted the wife of the patient 15 minutes prior to the bronchoscopy as he already spoke to her in person the day before. He received no answer from her so then he contacted the son of the patient. Again, there was no answer. As by normal protocol he waited 5 minutes post the scheduled time for the bronchoscopy but still received no answer. Unfortunately, due to no consent given, the bronchoscopy would have to be delayed to another date. It was urgent the patient needed a bronchoscopy but it was not emergent. Only if it is emergent would it be legal for the physician to override the unanswered consent and perform the bronchoscopy as the wife did allow for invasive procedures on the patient.
I was fortunately able to see one bronchoscopy today which the doctor was very informative to me throughout the procedure of what I was seeing on the monitor. Shadowing the Respiratory Therapists was also very interesting, however, due to the Respiratory Therapists having two students shadowing her, I was unable to have very many things explained to me. I completely understand the circumstance, and she was kind enough to realize I was not getting the full experience and let me shadow a free therapist. It is unfortunate I am not able to spend more than one day at the ICC as I definitely did not see all of the procedures a Pulmonary Disease Specialist would do. And, considering the PDS was very kind and outgoing, I am sure I would have learned much from shadowing for a couple of days. I am glad I was able to experience what I can though!
